“`html
Why Vertigo Hits Hard in Military Flight Training
I spent months interviewing military flight instructors before I understood why spatial disorientation kills more student pilots than mechanical failure. It’s not the vertigo itself—it’s what happens in the 6 to 8 seconds after it hits.
When you enter a steep turn or roll inverted, your inner ear (the vestibular system) sends signals to your brain about your body’s position in space. But at 6 Gs, accelerating through a barrel roll at 300 knots, those signals become noise. Pure contradiction. Your body screams “nose down” while your instruments say “wings level.” That gap—that sensory conflict—is where pilots lose the fight.
Here’s what actually happens in those critical moments. Blood pools in your extremities. Vision tunnels down to a pinhole. You feel like you’re spinning when you’re perfectly level, or perfectly level when you’re dropping toward the ground at 500 feet per minute. The F/A-18 pilot with 800 hours and the 19-year-old student? Same physiology. Same problem. The difference comes down to what they do in the next three seconds.
Spatial disorientation has been the leading cause of military aviation mishaps for over a decade—not weather, not engine failure, not traditional pilot error. The Navy’s own data shows it accounts for roughly 7% of all mishaps. But in training flights with students below 300 hours? That number jumps to 12%. Probably should have opened with this section, honestly—the stakes are why the recovery method exists at all.
The Cross-Check Method Instructors Teach First
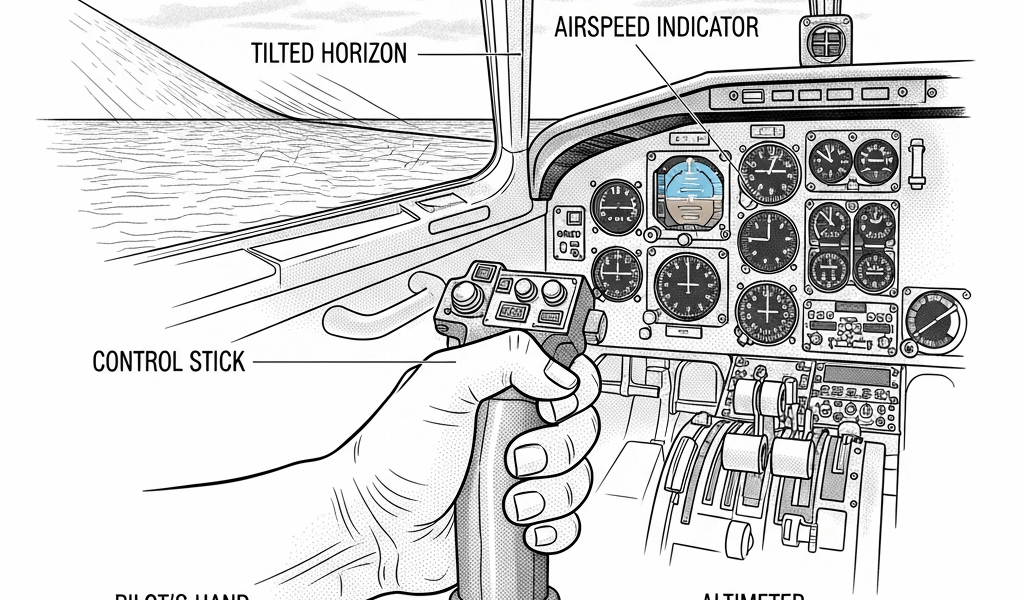
Every military flight school in the US teaches the same four-point scan. Airspeed. Altitude. Attitude. Heading. In that order. Every single time.
I watched an instructor at Columbus Air Force Base walk a student through this after a rough spin recovery. The student’s hands were shaking. The instructor didn’t rush.
“Your inner ear is lying to you right now,” the instructor said. “Your instruments are not. Look here first—airspeed. What does it say?”
Airspeed is step one because it’s the hardest to fake. A spinning aircraft has a specific airspeed signature—drop in the numbers, and you’re in an uncontrolled spin. Normal or climbing airspeed means you’ve already recovered, even if your body doesn’t believe it yet. This single number tells your brain something is actually happening. It anchors you to reality.
Altitude comes second. This is survival—you need to know how much sky you have left. A student in disorientation often feels high when they’re low, or senses a climb that’s not happening. Altitude tells you the truth about your remaining options.
Attitude indicator is next. This is the one that fights your inner ear directly. It’s a small gauge—looks like a tiny airplane inside a circle with a horizon line. When that instrument says you’re wings-level and your body says you’re upside down, you have to make a choice. Pilots choose the instrument. Every time. This mental shift saves lives.
Heading last. Once you know you’re safe—airspeed normal, altitude sufficient, attitude controlled—then you navigate.
Here’s a real scenario an instructor shared. A student pilot is inverted in a steep spiral. The G-forces are pulling at 5.5 Gs. Vision is tunneling. The student’s inner ear screams that the horizon is rotating clockwise, faster and faster. The brain demands action. Every instinct says “pull back on the stick to get level.”
Pulling back while inverted tightens the spiral. This is where the cross-check becomes a lifeline.
Eyes to airspeed: still climbing, holding 250 knots. Eyes to altitude: 3,000 feet, losing 500 per minute. Eyes to attitude: showing inverted, wings level. Eyes back to airspeed.
The student’s hands follow the instruments, not the inner ear. Roll wings level first. Then pitch up. Airspeed bleeds to 200. Altitude steadies. The spiral stops. The student is flying again—not by feeling, but by reading.
Why this order works: it interrupts the feedback loop that amplifies panic. By forcing your eyes to external data in a specific sequence, you bypass the sensory conflict. Your vestibular system is still sending false signals, but you’re not making control inputs based on those signals anymore. You’re making inputs based on facts. The disorientation continues for maybe 30 more seconds—the student still feels sideways—but the aircraft is safe. That’s the entire goal.
Recovery Techniques Used in High-G Training
The cross-check is mental. Recovery techniques are physical. Experienced pilots told me the difference between these two approaches matters far more than people realize.
Breathing first—when vertigo hits, pilots naturally hold their breath or breathe shallow. Oxygen to the brain drops. Disorientation deepens. Instructors teach a specific rhythm: breathe in for 4 counts, hold for 2, breathe out for 6. Mechanical? Yes. But the point is to interrupt the panic response. A pilot executing controlled breathing is a pilot focused on execution, not on the sensation of spinning.
Body position and muscle tension come next. Fighter pilots ride G-suits—inflatable bladders that wrap around the legs and abdomen, preventing blood from pooling during high-G maneuvers. The suit isn’t a cure, though. You still have to tense your core muscles, squeeze your thighs, flex your arms. An experienced pilot doing a 7-G turn is performing isometric exercise while flying. Your muscles counteract the G-force, keeping blood in your upper body and head. Without this effort, blackout follows disorientation. With it, you stay conscious and in control.
Focus point selection surprised me when an instructor explained it. It’s about “choosing a reference point on the instrument panel and never letting your eyes leave it unless you’re executing the scan.” If your eyes wander during disorientation—searching for relief, following the motion you feel—you lose the scan. The cross-check collapses. But if you pick a single gauge, usually the attitude indicator, and hammer it with your gaze, your brain eventually accepts what your eyes are telling you over what your inner ear is telling you.
Mental imagery works too. Before a flight, instructors have pilots visualize disorientation scenarios and their response. See the spin. Execute the scan. Picture the nose dropping. Hands move to neutral. Visualize the recovery. This sounds like sports psychology because it is. Your brain doesn’t distinguish sharply between vivid imagination and reality. When the real spin happens, your muscle memory and neural pathways have already been primed. You respond faster. Fear response delays.
A former T-38 instructor I spoke with—2,400 hours logged—told me she still uses the breathing rhythm before a high-altitude sortie. “After thousands of flights, I don’t get vertigo anymore. But my body still wants to panic in certain situations. The breathing keeps me calm. The calm keeps me scanning. The scanning keeps me flying.”
Building Mental Resistance Over Time
Overcoming vertigo isn’t an on-off switch. It’s a progression across hours and exposure.
Students start in the simulator. No G-forces. No real danger. Just the sensation of disorientation in a controlled environment where they can practice the scan 50 times before leaving the ground. Modern full-motion sims pitch and roll with hydraulics—instructors can induce spatial disorientation algorithms that make even experienced pilots uncomfortable. But there’s a safety net. A student can fail a simulated recovery 10 times without consequence. This permission to fail is critical. Fear of failure delays adaptation.
Then basic aircraft maneuvers at altitude: shallow turns, climbs, descents. G-forces are light—maybe 1.5 Gs. Disorientation is minimal. The student learns to trust instruments in low-threat scenarios.
Weeks later come barrel rolls, loops, inverted flight. G-forces climb to 3, then 4. Disorientation becomes real. But the student has logged 15-20 hours of scanning already. Muscle memory is building. Confidence accumulates.
Months into training: spins, spirals, advanced maneuvers at 6-7 Gs. Serious disorientation. But now the student’s brain has been repeatedly exposed to the disconnect between inner ear and instruments. Neurologically, the brain has learned to weight instrument data more heavily. The contradiction still exists, but it triggers the scan instead of panic.
Confidence is the engine driving this progression. A student who believes the cross-check works executes it faster under stress. A student who doubts the method hesitates, loses focus, reverts to sensory input. Instructors spend as much time building confidence as teaching technique.
Fear of failure is the other factor. Military flight training has washout rates—not every student earns wings. This creates pressure. A student struggling with disorientation sometimes hides it from instructors, tries to tough it out alone, and ends up in a high-threat situation they’re unprepared for. The best programs normalize the struggle and emphasize that asking for help is a sign of maturity, not weakness.
When to Tell Your Instructor You’re Struggling
Not every pilot recovers at the same rate. This is not a failure.
Some students adapt in 20-30 hours. Others need 60-80. A few need 100+ before spatial disorientation stops triggering panic. Variation is normal. The risk is silent struggle.
If you’re a student and the scan isn’t clicking yet—if you’re still defaulting to inner ear signals during high-G maneuvers—tell your instructor today. Not after the next flight. Not after you “figure it out.” Now. Instructors have tools: extra simulator time, reduced-G progression, spot checks with instrument-only flying (hood work, where you fly on instruments with no outside references).
Red flags that signal you need immediate help: chronic nausea that persists beyond the flight, disorientation that doesn’t resolve even after recovery maneuvers, severe anxiety about entering certain maneuvers, or a feeling that the scan “isn’t working” no matter how many times you execute it. These can indicate medical factors—inner ear infections, fluid buildup, medication interactions, dehydration—that require evaluation by flight medicine.
Normal adaptation lag looks different: mild nausea that resolves within an hour, disorientation that clears the moment you complete the recovery, hesitation on the first few spins that disappears after repetition, anxiety before difficult maneuvers that eases once you’re executing.
The honest truth—some pilots discover they have a medical condition that affects vestibular function. Some realize they’re better suited to aircraft types that don’t require high-G training. Neither outcome is failure. Flying is unforgiving, and self-awareness is the only insurance policy you have.
The instructors I spoke with—the good ones—want their students to report struggles. A pilot who can’t overcome disorientation and hides it becomes a risk to everyone in the airspace. A pilot who asks for help becomes a pilot who knows how to solve problems. In combat, that’s the difference between coming home and not.
“`


Leave a Reply